Performed by Dr. Apurva Patel, Orthopedic Surgeon in Ahmedabad
Patient’s Problem
Mrs. Dhruvi(Name Changed for Privacy), a 28-year-old female patient (dominant left hand), reported to the Orthopaedic Department with
- Severe, constant left wrist pain for 8 months
- Dull, aching pain aggravated by daily activities such as holding a bowl, combing hair, and cleaning
- Marked stiffness and restricted wrist movements
- Weakness in the wrist and reduced function affecting daily life
- High VAS pain score: 9/10
- No history of trauma or systemic illness
The patient feared progressive disability as wrist strength and function were deteriorating.
Diagnosis
After detailed clinical examination and radiographic imaging, the following were confirmed:
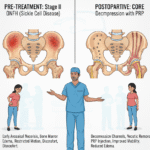
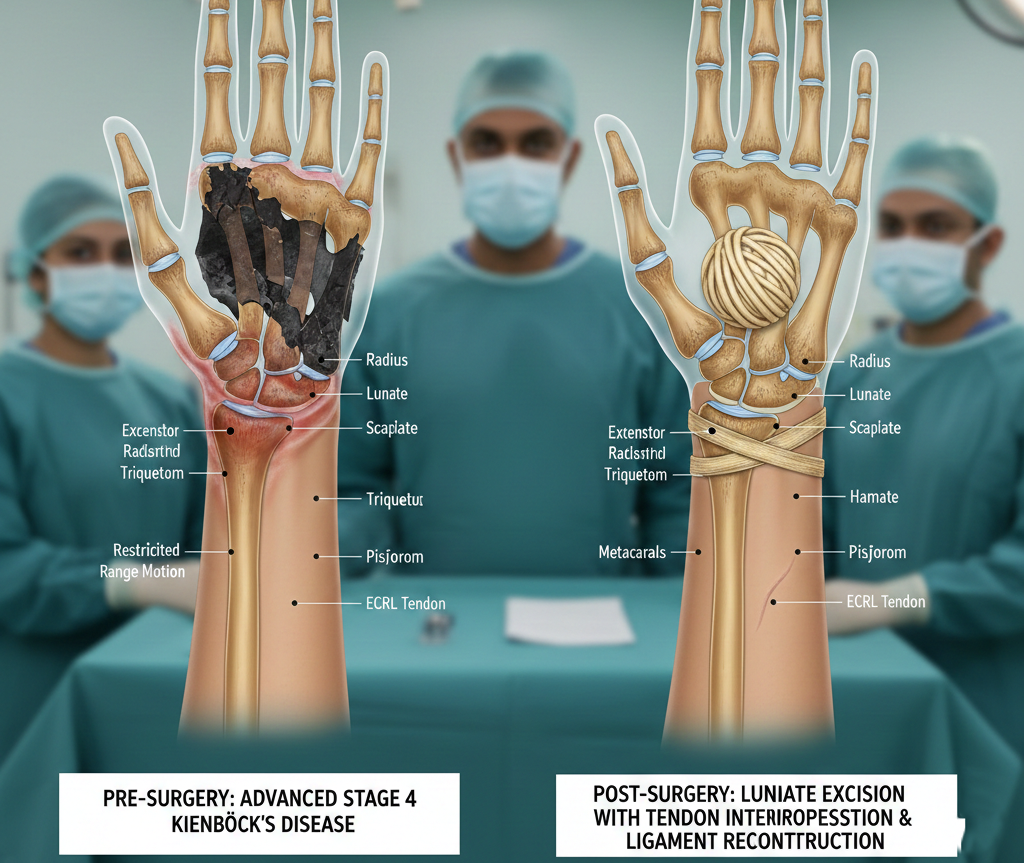
- Stage-4 Kienbock’s Disease (Avascular Necrosis of the Lunate)
- Fragmented and collapsed lunate
- Painful, restricted palmar and dorsiflexion
- Weak grip strength
- Significant functional limitation
Since the disease had already reached an advanced stage (Stahl Stage 4), conservative management or simple procedures were no longer adequate. A biological, stable, and long-term surgical solution was required.
Operating Team
The treatment was performed by the Orthopaedic Unit at SBKS MI & RC, India, and the research paper lists the following authors/clinicians:
1. Dr. Sarvang Desai — Professor & Head of Department (HOD)
- Senior-most consultant in the case
- Oversaw clinical evaluation, diagnosis, surgical planning, and postoperative supervision
2. Dr. Apurva Patel — Junior Resident (Corresponding Author)
- Assisted in clinical work-up
- Actively participated in operative steps
- Documented the case and follow-up
- Primary author responsible for the case report’s scientific preparation
3. Dr. Malkesh Shah — Associate Professor
- Assisted in surgical decision-making
- Provided intra-operative guidance
- Contributed to postoperative evaluation and literature review
All three doctors contributed collaboratively to the surgical and academic aspects of this case, as noted in the research paper.
Treatment Performed
Lunate Excision with ECRL Tendon Ball Interposition & Ligament Reconstruction
This novel biological reconstruction technique, performed according to the method described in the published research, involved the patient’s own Extensor Carpi Radialis Longus (ECRL) tendon.
Surgical Steps (From Research Paper)
- A transverse dorsal incision was made over the wrist
- The wrist capsule opened in a U-shaped manner
- Lunate bone excised piecemeal to remove necrotic fragments
- ECRL tendon harvested from the middle one-third of the forearm
- The tendon is split into two:
- One-half is used to create the coiled tendon ball
- The other half is used as a ligament-reconstructing tendon strip
- 2.7 mm holes drilled in the scaphoid and triquetrum
- Tendon strip passed through both bones to recreate:
- Scapholunate ligament
- Lunotriquetral ligament
- The coiled tendon ball is inserted into the space left by the excised lunate
- Tendon strip sutured on itself with Prolene
- The remaining half of the tendon returned to its native insertion
- Closure followed by below-elbow cast protection
The ECRL tendon was chosen because it is:
- Longer
- Thicker
- Provides better stability than Palmaris Longus
- Helps prevent further proximal row collapse
Postoperative Recovery & Follow-up
Before Surgery
- VAS pain score: 9/10
- Severe pain during routine tasks
- Wrist instability
- Restricted ROM
- Weak grip strength
After Surgery (12-Month Follow-up)
- VAS pain reduced to 1/10
- Improved grip strength
- Good wrist mobility
- Pain-free daily functional activities
- No carpal collapse or instability on imaging
- Patient regained confidence in using her dominant hand
This confirms that the ECRL tendon serves successfully as:
- A biological spacer
- A stabilizing ligament reconstruction
- A long-term solution for late-stage Kienbock’s disease
Conclusion
The collaborative work of Dr. Sarvang Desai (HOD), Dr. Apurva Patel (Junior Resident), and Dr. Malkesh Shah (Associate Professor) demonstrates that:
ECRL Tendon Interposition with Ligament Reconstruction
It is a highly effective, biologic, cost-efficient, and durable treatment option for late-stage Kienbock’s Disease.
This technique:
- Restores carpal stability
- Reduces pain dramatically
- Improves wrist function
- Avoids complications seen with silicone prosthesis
- Maintains long-term wrist biomechanics
The case highlights how an expertly planned and precisely executed biological reconstruction can restore pain-free movement and functional independence in patients with advanced wrist pathology.